




































Varicose veins are a disease associated with an increase in length, the formation of pathological serpentine rotations of the veins, irreversible saccular enlargements of their lumen, and insufficiency of the valves. The organs of the lower pelvis are involved in the process of varicose veins. The mechanisms of disease development are different. Physicians include the perineal region, external and internal genitals as atypical localizations.
General information about the pathology
The process of blood flow through the veins continues in such a way that, under physiological conditions, preconditions are created for the development of stagnation and blood flow.
Varicose veins of the vulva (VV) - vasodilation of the external genitalia. The disease occurs in women suffering from varicose veins of the pelvis and legs, as well as in pregnant women. In 30% of cases, pelvic varices include the perineum and vulva.
The start of treatment of the disease is delayed due to the location in an intimate place. Women are shy. In some cases, patients do not experience pain or discomfort. But labial varicose veins during pregnancy and not only during the carrying of a fetus continue with complications: blockage of the veins by a thrombus (thromboembolism), disorders of sexual sensitivity, pain in the perineum, psycho-emotional problems and family conflicts.
The mechanisms of occurrence of pelvic vessel overload have not been fully elucidated. The cause of the primary form of the disease is called a malfunction of the gonadal (ovarian) vein valves. This provokes a backflow of blood and increases the pressure in the venous nodes of the lower pelvis. Valve insufficiency can be acquired or congenital. Worsens with age or pregnancy.
The secondary form of VVV of the pelvic organs is associated with gynecological pathology: endometriosis, tumors of the pelvic organs.
Diagnosis of the disease is difficult due to the fact that there are no specific symptoms of its course. It is based on the results of ultrasound (ultrasound).
To distinguish primary and secondary forms of pathology, Valsalva test is used during sonographic examination. With a secondary cause of pelvic varicose veins, it is negative.
Varicose veins of the labia with VBT
To establish a diagnosis of varicose veins of the labia, a doctor's examination is required. The symptoms of the disease are as follows:
- varicose veins in the genitals;
- pain in the external genital area;
- a feeling of heaviness and burning in the perineum;
- swelling of the perineum by the end of the day.
Chronic pelvic pain occurs less frequently (in 30% of cases).
After establishing the diagnosis, a study is performed to identify the degree of complexity of the pathological process and to prescribe adequate treatment. A series of events were held:
- ultrasound examination of perineum and leg veins - USAS;
- performing ultrasonography of pelvic vessels, including vaginal, uterine, parametric, ovarian, iliac, inferior and renal vena cava;
- according to the indications, multispiral computed tomography (MSCT), selective ovarography and pelvic phlebography (SOFT) are performed.
Doctors call it a characteristic feature of varicose veins in the lab with VBT that the disease is progressing steadily and combined with the transformation of intrapelvic veins.
Treatment of varicose veins of the vulva with varicose veins of the lower pelvis
Treatment IV is prescribed based on symptoms and diagnostic results.
In complex drug therapy for the treatment of chronic systemic venous pathology, nonsteroidal anti-inflammatory drugs and phlebotropic drugs are prescribed.
Prescribe pharmacotherapy with antiplatelet agents, intrapelvic block with antihypoxants, ultrasound physiotherapy, therapeutic exercises. Antioxidants and enterobiotics are added to the therapy.
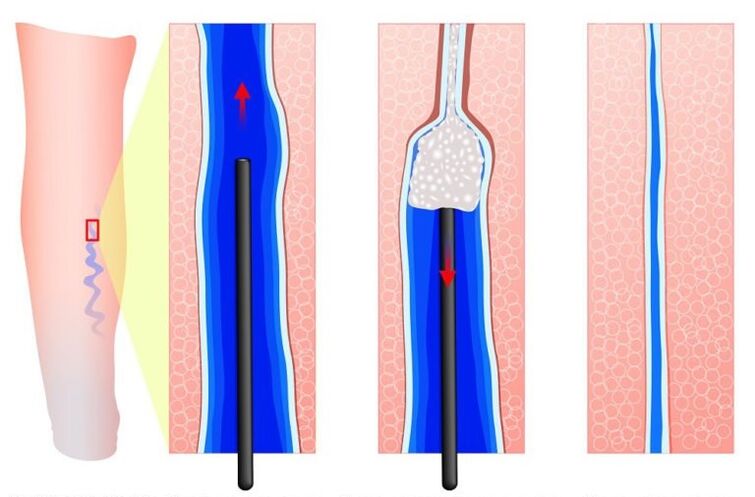
According to the indications, phlebosclerotic treatment - sclerotherapy is performed. The ship is "closed" with drugs and lasers. It stops working. The procedure does not use special anesthesia methods. It is performed on an outpatient basis and produces a cosmetic effect.
With the abundance of pelvic veins, dilation and return of blood through the gonadal (ovarian) veins, a surgical operation to remove the veins is indicated. In the case of varicose enlargement of the labia minora, it is removed.
Varicose veins of the vulva during pregnancy
Pregnancy is the first most common risk factor leading to the onset of VVV. A significant and steady increase in progesterone concentration already in the early stages of pregnancy reduces venous tone and worsens impaired blood flow. Also, VBT, which includes the perineum and vulva, is associated with compression of the large veins of the retroperitoneal region (iliac veins and inferior vena cava) by the pregnant uterus.

Doctors recommend compression garments during pregnancy.
Often varicose veins of the vulva occur bilaterally. Signs of the disease:
- a marked increase in vulvar veins over a period of 18-24 weeks during the first pregnancy, from 12 weeks with a recurrent pregnancy;
- groin discomfort;
- traction, pain, dull ache in the pelvic region;
- pain during intercourse;
- pruritus of the vulva;
- swelling of the genitals and perineum.
Signs of pathology progress with the course of pregnancy. In addition to increasing the size of varicose veins, its compression is determined by the third trimester. A characteristic symptom of IV is its combination with inguinal varicose veins during pregnancy or varicose veins in the legs.
Instrumental examination of varicose veins of the labia in pregnant women is limited to their ultrasonography, as well as to ultrasonography of the legs, because the painful changes in the venous bed undergo involution in the postpartum period.
In most cases (about 80%), from the first days of birth, the symptoms of varicose veins during pregnancy begin to subside and are minimized 2-8 months after the baby is born. A complete return of the vessels diameter to their original values does not occur.
In 4-8% of women, IV does not disappear after birth and the disease progresses.
An interesting feature is the relationship between the end of the feeding period or the reduction in the volume of breastfeeding with the rate of disappearance of varicose veins in the groin in women. A shortened lactation period is associated with reduction and disappearance of varicose veins and vice versa. This proves that varicose veins of the perineum during pregnancy are associated with a change in hormonal levels.
Treatment of varicose veins of the perineum during pregnancy
The basis of therapy for varicose veins during pregnancy is phlebotropic treatment. In the majority of fertile women, IV begins in the II and III trimester. Diosmine preparations may be used during this period. The severity of the pathology symptoms is reduced by the purified micronized flavonoid fraction. Itching is relieved by zinc paste and H1-histamine receptor blockers.
Low molecular weight heparin in a prophylactic dose prevents venous thrombosis and pulmonary embolism (blockage of blood vessels).
As an option for treating compression, it is prescribed to wear tight elastic underwear using latex cushions or gauze. Relieves puffiness of lips and feeling of heaviness. Special compression vest for women with vulvar varicose veins helps a lot.
If a complication develops, such as local thrombophlebitis, surgical treatment is required.
When a conglomerate of varicose veins is found in the genitals, the question of how to give birth arises. Natural childbirth is allowed with varicose veins of the vulva. Conversely, the risks of surgery during a cesarean section are higher than the onset of bleeding from painful vessels during childbirth. This rarely happens. But with varicose veins of the vagina, a cesarean section is often done.
Prevention of varicose veins of the labia
The main factor in the formation of varicose veins in the groin is the retention of the fetus. It is difficult to mention any method of prevention, given the fact that during pregnancy there are a number of limitations to many therapeutic measures. Some tips to follow:
- exclude physical and static stress;
- follow a diet;
- perform therapeutic exercises, in which movements accelerate blood flow from the legs and lower pelvic organs;
- in case of cessation of venous work, the presence of varicose veins before pregnancy, it is necessary to take phlebotropic drugs, wear compression underwear.
An effective method of prevention is considered to be an operation on the ovarian veins, surgery for other pathologies related to varicose veins. This reduces the phenomenon of pelvic venous congestion, reduces the risk of varicose veins in the labia.
Varicose veins of the vulva is a common disease in women with varicose veins of the pelvis, legs or during pregnancy.
To improve the quality of treatment of patients with chronic venous disease, it is important to detect the disease, to distinguish between methods of diagnosis and treatment of this condition.